In summer 2023, Dundee medics Angus, Jed, Lee and Jack spent 4 weeks at the health post LED supports in Quisuar, in Peru’s Cordillera Blanca. Here are the write ups from Angus and Jed (including PDF originals), together with some of their photos. Thank you all for all your hard work in Quisuar and surrounding villages. It sounds like you had a great time!
Rural Medicine in the Cordillera Blanca Mountains, Peru – Angus Pinsky
Placement
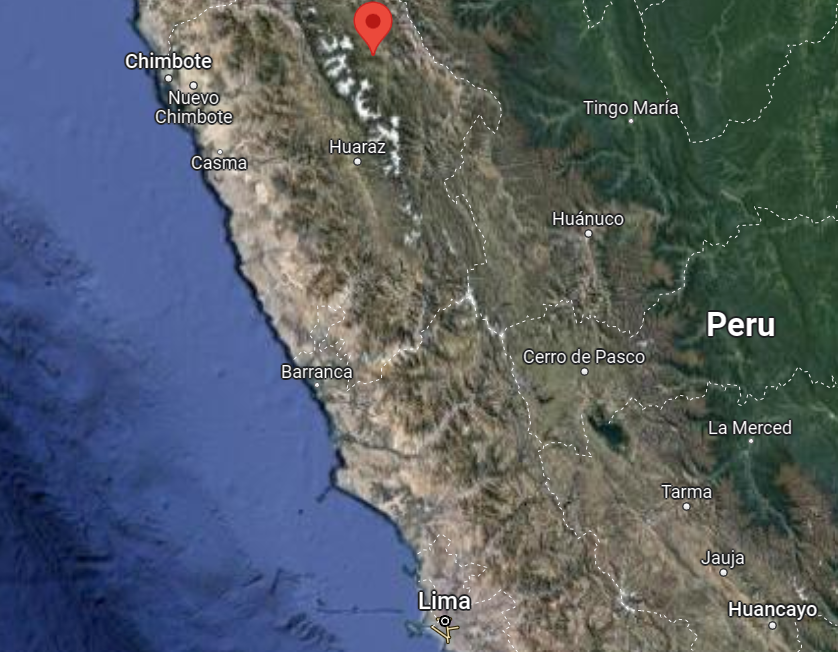
We spent four weeks volunteering in the north of Peru, in a health post in the Cordillera Blanca mountains, and in the town of Acopampa, in the northern province of Carhuaz.
The health post is run by the small charity Light Education Development, located in the village of Quisuar. It is staffed by a single nurse, and we were also accompanied by a friendly guide/translator, called Juan. Here we ran clinics for the local people, who visited from the surrounding villages. We could take histories, perform physical examinations, and prescribe from the post’s small medication store (to which we contributed some donated medicines). The local people speak Quechua, and so we had to translate throughout each consultation. Each day we would see up to 25 patients, although the number of patients who visited the post would vary greatly, and they would arrive anytime between 7am and 10pm.
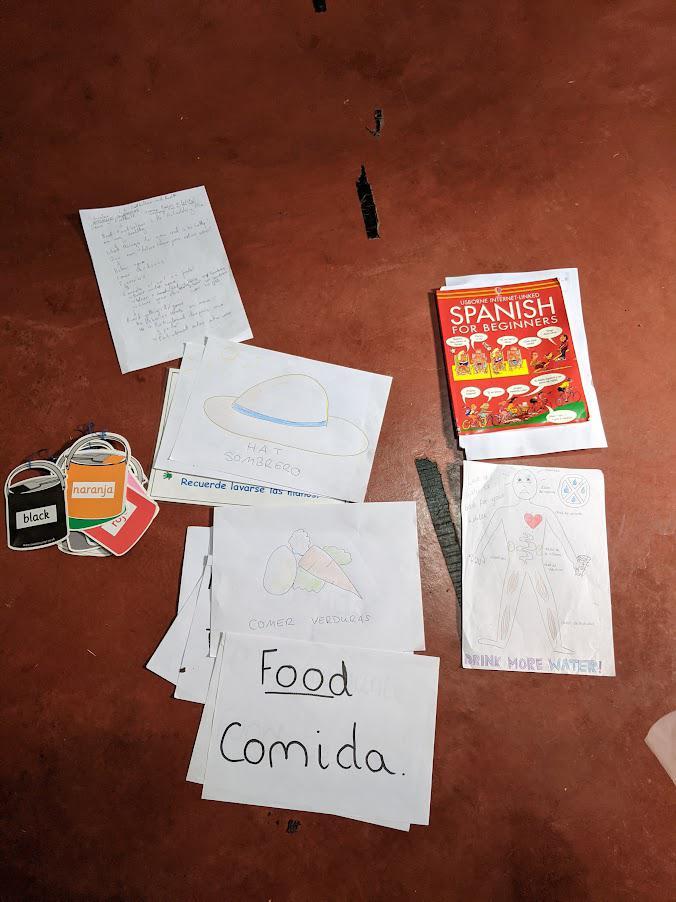
The ailments we witnessed most often were common conditions, such as UTIs, URTIs and GORD, as well as chronic conditions such as osteoarthritis. There was a distinct lack of public health knowledge, meaning our primary role was often educating patients on concepts such as curative vs symptomatic treatment, eating healthily, and drinking adequate quantities of water.
Alongside our general consultations, we also provided basic vision assessments and free reading or distance glasses for those who needed them.
In Acopampa we performed basic vision assessments on all the pupils at a local school, as well as some parents and teachers. Here we also provided free glasses, that had been donated to the charity.
Peru
Peru is a high-middle income country, located on the west coast of South America. It has a population of 33.72 million, and the capital is Lima.
Healthcare in Peru is provided by a mix of government and private organisations, with an insurance-based model. A majority of citizens receive some form of government coverage. However, there are many barriers to accessing healthcare, especially for those in poverty and those who live rurally. We witnessed this during our time in Quisuar, where the villagers who visited us would have otherwise had to travel a long distance to reach the nearest government- run health post, and even further for any specialist care. There are also difficulties for Quechua-speaking communities, as consultations are generally conducted in Spanish.
Organisation
In order to organise our elective, we got in touch with Light Education Development through the contact form on their website, which can be found here:
https://lighteducationdevelopment.org
We were then contacted by Val, the charity’s founder, who was our supervisor.
Pros
- Exposure to health practice radically different to that found in the UK
- Good immersion into the lifestyle and culture of local people
- People were always friendly, welcoming, and immensely grateful
- Program established based on a thorough understanding of local needs and issues
- Health post based in a strikingly beautiful mountainous region of Peru, well off the tourist track
- Opportunity to take on a lot of personal responsibility vs a more conventional placement
- Opportunity to travel in Peru, see Machu Picchu, and lots of other amazing sights
- Cost of living is very cheap compared to the UK
Cons
- Language barrier if you don’t have pre-existing Spanish knowledge
- Only basic amenities at the post, which could be challenging for those not prepared for a pared-back lifestyle akin to camping
- Could be lonely without a group
- Have to go through around a week of adjustment to altitude to avoid altitude sickness, as the post is located at around 3000m elevation
Tips
- Learn some Spanish!
- Take a four-season sleeping bag, comfy mat, and a water-filter
- Speak to someone who has been before about practicalities (I have a packing list I can pass on)
- Follow all the advice of the local guide
- If you’re interested in trekking, let your guide know
Quisuar Health Post Report – Jed McIntyre
Volunteering in the Quisuar health post was something truly special. Better than just visiting Peru, working rurally in the mountains made us a part of the community for our time spent there and our welcome couldn’t have been warmer. Our days were kept busy and entertaining running clinics as a team, which consisted of ourselves (5th year students), Juan who acted as our translator/guide and the health post nurse. As students, the exposure and opportunities on this trip was invaluable and helped develop confidence in leading consultations as well as general medicine. From initial presentation to examination and management it was all student-led, great to get a taste for responsibility and we never felt too far out of our comfort zone. We saw a wide range of conditions from many specialities including arthritis, viral coughs, angina, UTIs and vision problems. This healthcare was a huge benefit to patients and with the community being so small, being able to see the impact felt great, from clearing up diseases to providing glasses – this was huge for quality of life as being able to see well enough to thread a needle is very important to the families.
We ran clinics from Quisuar offering our services to the locals who really appreciated our time. It always felt useful contributing our medical management as well as just information which meant a lot to patients who had worries or questions. We also took a couple visits to the neighbouring localities of Seccha and Pochgoj where we were put up in accommodation and held clinics for a slightly larger population of people. This was also where we were able to stock up on biscuits! These journeys gave us opportunities to see more patients and work as a more mobile unit of healthcare. Although our stay here had wifi it couldn’t match the beauty of our surroundings in Quisuar, at ≈2900m elevation the mountain landscape was breathtaking and so isolated.
We also loved the opportunity to get involved in the community by teaching English and running activities with the local kids some afternoons as well as joining in sport festivals who were always keen for some extra numbers to play football or volleyball. Along with my memories of our exciting clinical work and the beautiful location, I’ll never forget Jack’s flying volley from the halfway line to raucous applause from the crowd. My hero.
Our time in Quisuar offered a unique chance to visit the beautiful country Peru, to learn and develop our knowledge and skills in a new environment. And to contribute to and belong in a community on the other side of the world. To experience their hospitality, stories and culture was a treat!
Photos









If you’re a medical student interested in spending your medical elective at the Quisuar Healthpost, check out our How you can help page for more details.